

Implicit in this question is whether saturated fat consumption should be restricted; an overlooked aspect of that debate is that avoiding mortality should not be the primary goal of a diet. There are aspects of foods besides their effect on mortality that are relevant to whether or not they should be consumed: their taste, cost, and effects on broader well-being. That aside, it is something that is worth studying for the sake of truth, particularly for those who are in poor health.
Besides that, there is also the question of the outcome variable: ideally, it would be overall mortality, but evidence regarding the specific effect on certain types of deaths is useful for those who are genetically predisposed to them. In the case of SFA, the hypothesized mediator in the relationship between SFA intake and mortality is CVD; cardiac arrests are a fairly common cause of death, so an increase in CVD incidence is also likely to result in an increase in overall mortality.
Meta-analyses and literature reviews on the topic of SFA and CVD are a dime a dozen, so a few researchers decided to do a literature review of the literature reviews on the relationship between saturated fat and CVD.
Valk R, Hammill J, Grip J. Saturated fat: villain and bogeyman in the development of cardiovascular disease? Eur J Prev Cardiol. 2022 Dec 21;29(18):2312-2321. doi: 10.1093/eurjpc/zwac194. PMID: 36059207.
Methods and results: PubMed, Google scholar, and Scopus were searched for articles published between 2010 and 2021 on the association between SFA consumption and CVD risk and outcomes. A review was conducted examining observational studies and prospective epidemiologic cohort studies, randomized controlled trials (RCTs), systematic reviews and meta-analyses of observational studies and prospective epidemiologic cohort studies, and long-term RCTs. Collectively, neither observational studies, prospective epidemiologic cohort studies, RCTs, systematic reviews, and meta-analyses have conclusively established a significant association between SFA in the diet and subsequent cardiovascular risk and coronary artery disease, myocardial infarction, or mortality nor a benefit of reducing dietary SFAs on CVD rick, events, and mortality. Beneficial effects of replacement of SFA by polyunsaturated or monounsaturated fat or carbohydrates remain elusive.
Conclusion: Findings from the studies reviewed in this paper indicate that the consumption of SFA is not significantly associated with CVD risk, events, or mortality. Based on the scientific evidence, there is no scientific ground to demonize SFA as a cause of CVD. SFA naturally occurring in nutrient-dense foods can be safely included in the diet.

There is a consensus in favour of no effect of SFA on CVD.
This meta-review does not include the latest and largest meta-analysis on SFA intake and overall mortality, as their outcome variable is CVD:
Reynolds A, Hodson L, de Souza R, Tran Diep Pham H, Vlietstra L, Mann J. Saturated fat and trans-fat intakes and their replacement with other macronutrients: a systematic review and metaanalysis of prospective observational studies. Geneva: World Health Organization; 2022. Licence: CC BY-NCSA 3.0 IGO.
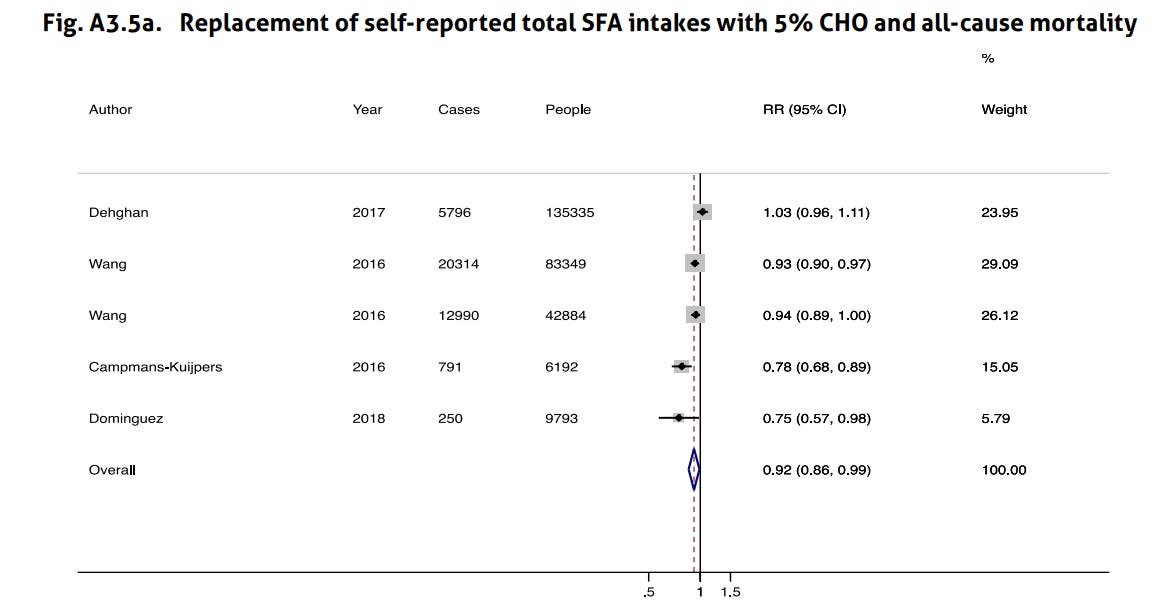
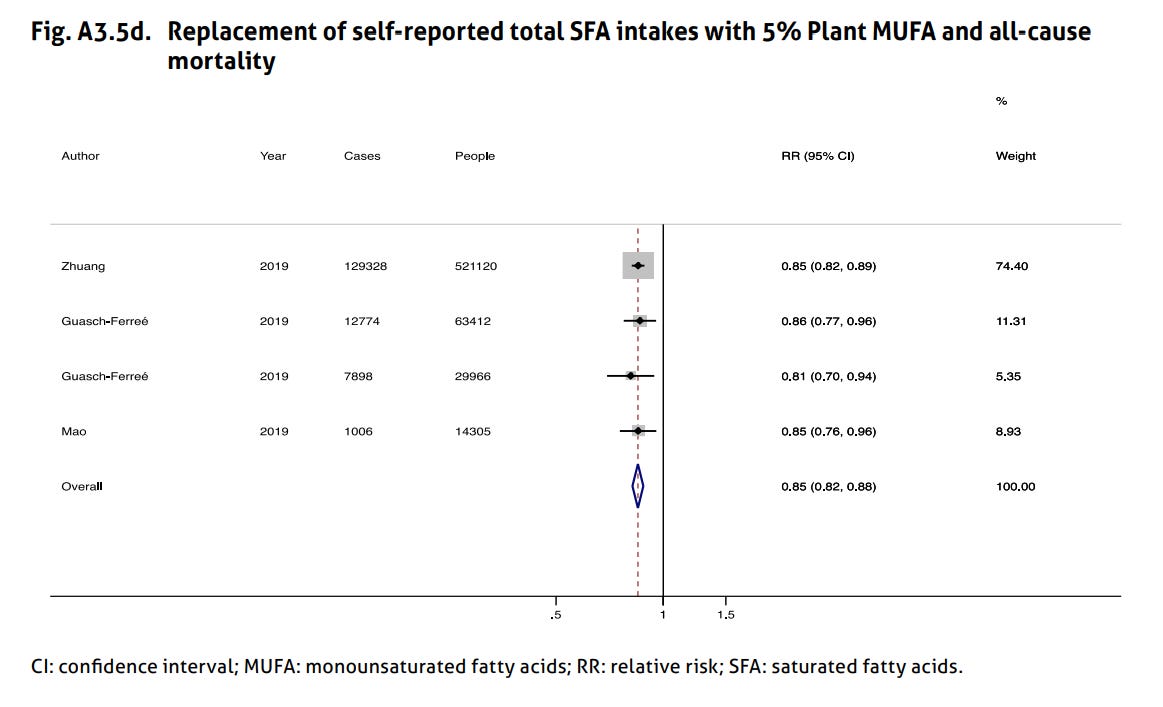
There were 112 publications (3 696 568 participants) relating to SFA and 55 publications (2 227 241 participants) relating to TFA and prespecified health outcomes. Higher dietary intakes of SFA were associated with increased mortality. Mortality reduced when 5% of total energy from SFA was replaced with polyunsaturated fats (PUFA; relative risk [RR] 0.85; 95% confidence interval [CI]: 0.75 to 0.97), monounsaturated fats (MUFA; RR: 0.84; 95% CI: 0.75 to 0.95), plant MUFA (RR: 0.85; 95% CI: 0.82 to 0.88) and carbohydrates (RR: 0.92; 95% CI: 0.86 to 0.99). Coronary heart disease (CHD) incidence reduced with a 5% energy replacement with PUFA (RR: 0.89; 95% CI: 0.81 to 0.98), plant MUFA (RR: 0.83; 95% CI: 0.69 to 1.00) and slowly digested carbohydrates (RR: 0.94; 95% CI: 0.89 to 0.99). Higher tissue measures of total SFA were associated with increased CHD and type 2 diabetes incidence. Higher dietary intakes of TFA were associated with increased mortality, CHD and cardiovascular disease. A 2% replacement of TFA with plant MUFA reduced mortality (RR: 0.90; 95% CI: 0.85 to 0.96) and CHD (RR: 0.80; 95% CI: 0.70 to 0.92). The certainty of evidence was graded from moderate to very low, largely due to the amount of data available.
These are their results regarding the association between SFA and all-cause mortality.

The link between self-reported SFA intake and all-cause mortality is not clear: the confidence interval contains 1 and there is large amounts of heterogeneity in effect sizes, even after removing outliers.
They also did a meta-analysis on the effect of replacing SFA with a different macronutrient type on mortality — as far as I can tell, the only replacement that is likely to work is replacing SFAs with plant-derived MUFAs. The other meta-analyses have high heterogeneity and confidence intervals that are too close to 1.



There is also the question of cross-national patterns, which were some of the evidence first used to justify the diet-heart hypothesis. Take, for example, the chart produced from the seven countries study:

Such a strong correlation is difficult to find by chance, but a recent assessment found a relationship in the opposite direction (?):

I’m more inclined to trust the latter finding as it comes from a more homogeneous region in terms of culture/genes/environment (Europe) and has more datapoints.
In all honesty, my intuition is not satisfied with the last chart either.
II.
Perhaps saturated fat causes the lipid profile to change in a way that helps the heart, making up for the increase in cholesterol levels.
Perhaps the effect SFA has on increasing HDL cholesterol makes up for the increase in LDL cholesterol, resulting in a null effect on heart health.
Perhaps foods with saturated fat make up for the negative effect on heart health by having other effects that are positive.
Perhaps studies based on self-reported intake are not powerful enough to find an effect.
Perhaps other macronutrients (e.g. PUFAs, carbs) also have adverse effects on health, which biases the relationship between SFA intake and mortality towards a null.
These are a list of potential explanations that I have come up with on why the evidence for the link between SFA and mortality is so weak. I don’t have any strong opinion on any of them; that said, I think that it is not prudent to advise the public to cut down on saturated fat intake.
Personally, I consume high levels of SFA (15-30% of energy?), and plan to replace with MUFA (not PUFA or carbs) when I get older, as I am genetically predisposed to having cardiac arrests.