
What is the optimal body type?

TL;DR:
The optimal body mass for the general population is somewhere between 19 and 22, though this optimum could vary between individuals based on their race and frame size.
The effect of being underweight on mortality is massively overstated by the correlative evidence, and having a BMI of between 17 and 19 is probably fine for most people.
Reasonable levels of muscularity and fitness are healthy.
Excess adiposity is unhealthy (who would’ve thought?)
Excess muscularity may be unhealthy.
The notion of an “optimal body type” is somewhat convoluted, as there are various mechanisms by which a body type could be considered the best. A body type may be the best because it is the natural result of eating habits and physical exercise that causes well-being and longevity, or it may be the best because the body itself has an effect on health. Different body types may also be best for different things: for example, a body with very low body fat will be very attractive, but might not be the best for health (spoiler: very low body fat is either optimal or at the very least not deleterious). Personally, I use mortality as a proxy for health, because it is the hardest indicator to fiddle with statistically.
Because high quality medical research is very difficult to come by, correlative or pseudocausal evidence must be used to determine the optimal body type. Of course, correlation doesn’t indicate causation, but in this specific situation it doesn’t matter very much. Say, for example, that the reason that adiposity is associated with mortality is because certain diets and exercise regimes are causal for mortality, and those practices also cause thinness. This doesn’t make much of a difference in terms of advice, because the same health practices would be pursued regardless of whether the relationship between adiposity and mortality is causal or not.
There is also the question of how to measure the optimal body — BMI is typically what is used because it is the most easy to calculate, but it has been subject to criticism because it is allegedly biased against both short people (short women in particular) and tall people according to different critics. The Rohrer school alleges that, because weight is associated with volume and not height, the optimal way to calculate it should be kg/m^3. However, this fails to take into consideration that because of regression to the mean taller people tend to have smaller frames, so the measurement would need into consideration. Statistical analysis that attempt to calculate the optimal superscript suggest that it is roughly 1.9 in men and 1.5-1.9 in women [1], [2], indicating that the traditional superscript of 2 probably works fine.
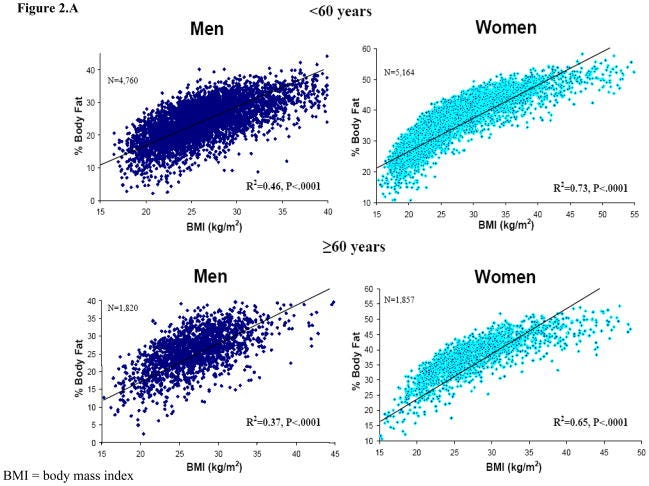
Statistically speaking, BMI correlates at 0.68 with body fat % within men and at 0.85 within women — not great, but still worth using. BMI is also very easy to measure, so naturally there are more datasets that have it than better measurements, like waist circumfrence or body fat percentage.
II.
Within clinical or unhealthy samples, measures of minor obesity correlate positively with longevity, which has been dubbed the obesity paradox. Traditionally, there are three explanations for this paradox:
It is a collider bias that results from obesity causing increased levels of medical care independent of health.
The effect is due to reverse causation, where severe illness causes lower body weight.
The obesity is to an extent protective, and prevents people from dying from certain diseases.
There is a lot of evidence that suggests that either explanation 1 or 2 are true, and little if any evidence for explanation 3.
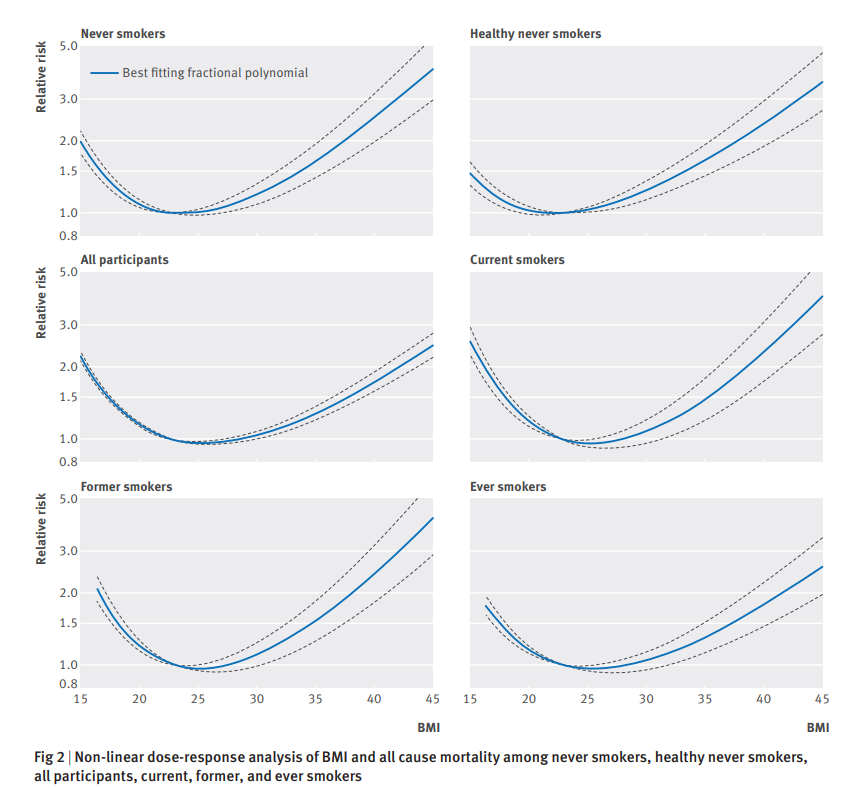
As the association between BMI and mortality becomes more plausibly causal (e.g. more factors are controlled for, or longer followups are used), the relationship between BMI and mortality becomes increasingly linear. Within the general population, the optimal BMI for risk of death seems to be about 25, however when the population is subsetted to healthy people who never smoke, the optimal BMI is about 22. The effect of being underweight is also severely reduced, with the relative risk of death for individuals with a BMI of 15 falling from 2.2 to about 1.5.
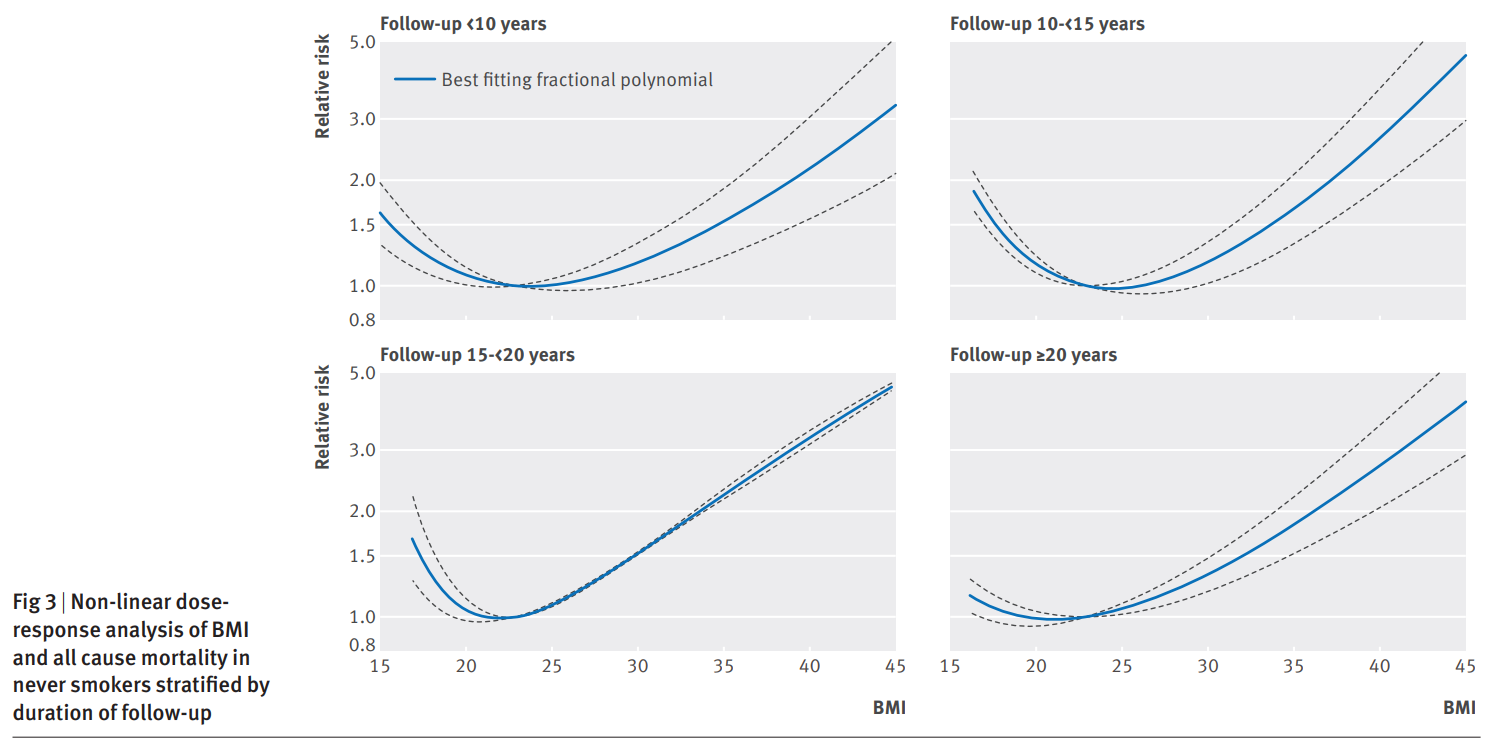
When followups that are done in under 10 years are compared to those done more than 20 years later the relative risk of dying within never smokers with a BMI of 15 falls from 1.5 to about 1.2, and the optimal BMI for longevity falls from ~24 to ~21. The same is not observed as robustly for the effect of major obesity — a BMI of 40 is almost always associated with a relative risk of about 40.
There are also some studies that attempt to assess the causal effect of BMI on mortality by using child BMI as a proxy for adult BMI that find the effect of relatively low BMIs (17-20) is greatly reduced.

I should note that this study design is not perfect, because the same illnesses that cause both death and low BMI may be inherited by children
To account for the independent effects of each type of mass, some researchers tried to predict lean and fat mass using biomarkers. Their predictions correlated with x-ray measurements at 0.95, so there is probably very little bias that results from using biomarkers as a proxy. Height was also adjusted for to avoid this factor from attenuating the effect of each type of mass.
They found that predicted fat mass has no effect on mortality between the ranges of 5kg and 21kg, and the relationship between lean body mass and mortality followed the conventional u-shape, where the optimal lean body mass was roughly 60kg.
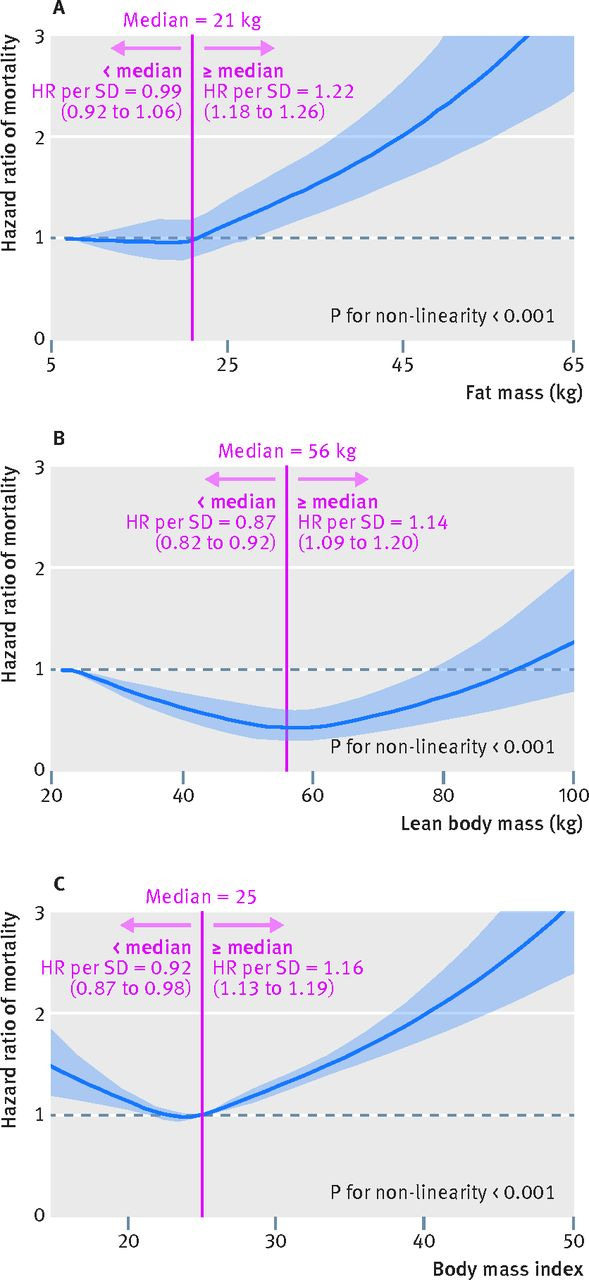
Because lean mass and fat mass tend to correlate, this suggests that the effect of low lean mass on elevated mortality and the effect of low fat mass on reduced mortality are actually understated, and the true effects are probably greater than this paper suggests. In other words, low lean mass is probably even more strongly causal for mortality, while low fat mass is a protective factor.
III.
Beyond body mass (which is a proxy for adiposity), there is also the question of whether having higher levels of muscularity or fat distributions is causal for greater levels of health.
Muscularity (as assessed by the ability to do pushups) strongly predicts cardiovascular disease - people who can do over 40 pushups are 96% less likely to have a heart attack than those who can only do between 0-10 pushups.
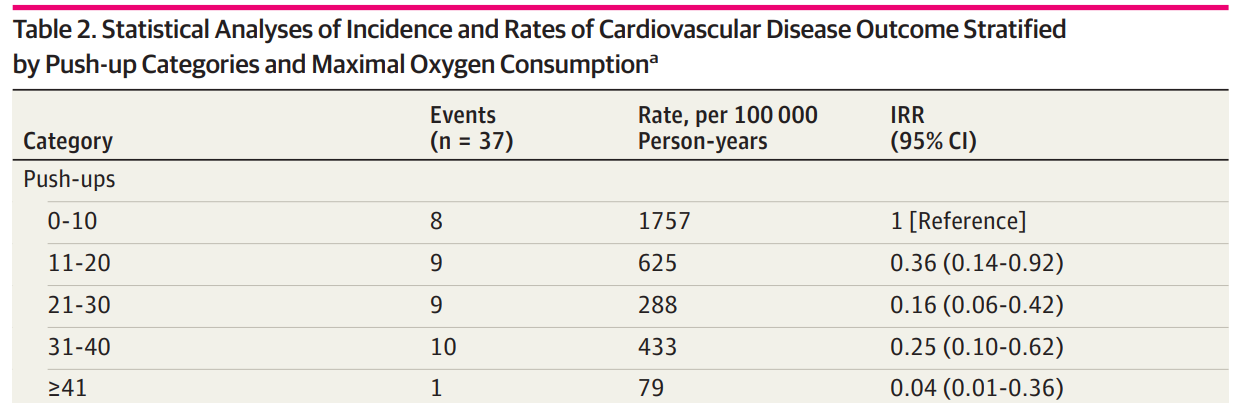
Normally, I would reject evidence like this. It’s within a relatively small sample (n = 1104) and only assesses one health outcome. However, the strength of the association is so large that you would have to be an idiot to ignore it.
There is also the standard correlative evidence, which suggests that skeletan/lean mass is associated with a lower risk of death even after BMI is controlled for, so most of the reverse causal effect of severe illness causing reductions in mass has been controlled for. Unfortunately, because health researchers insist on using quantiles, BMI is not perfectly controlled for, so there may still be some reverse causality within the observed relationship.
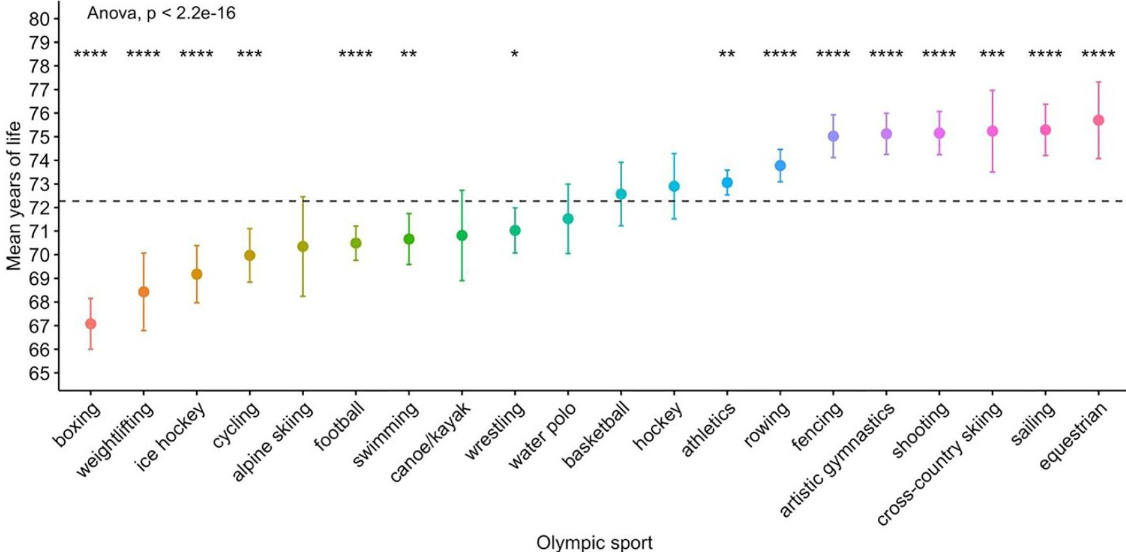
What is more interesting is not whether muscularity is health in general (it almost certainly is), but whether or not being too muscular is a health risk. Olympic bodybuilders tend to live shorter lives than other athletes, though this is potentially confounded by poor steroid use, as lifespan by sport largely seems to be a function of the potential for injuries and the amount of steroids that are used. Nevertheless, the fact that weightlifters are beat by cyclists and ice hockey players is still concerning.
There are multiple case studies (25) of prominent bodybuilders who died premature deaths. Of the 16 deaths for which a cause of death was available, 6 died of heart attacks. This is not much different from the 1/5 deaths that are supposedly caused by heart disease, which isn’t particularly strong evidence. This has not stopped the writers of that study from speculating that there might be something there; after looking through the paper, they don’t seem to favor the theory that anabolic steroids are the cause, instead they argue that the cause may be left ventricle hypertrophy which is caused by strenuous exercise.
What is my take on this far-out theory with no real evidence to back it up?
I believe it. For a simple reason. Huge bodybuilders look ugly. And if they look ugly, they are probably unhealthy. I don’t think it’s a coincidence that the most attractive BMI within women (19-20) is also the one that is the most causally optimal for longevity. To clarify what I mean by “excess muscularity” - this would be an example of a body that is too muscular:

This is probably fine:

There is also the issue of the distribution of fat around the body. As far as I know, there is no known way of changing the distribution of fat around the body besides surgical interventions and estrogen, which causes the body to store fat around the breasts, buttocks, and thighs.
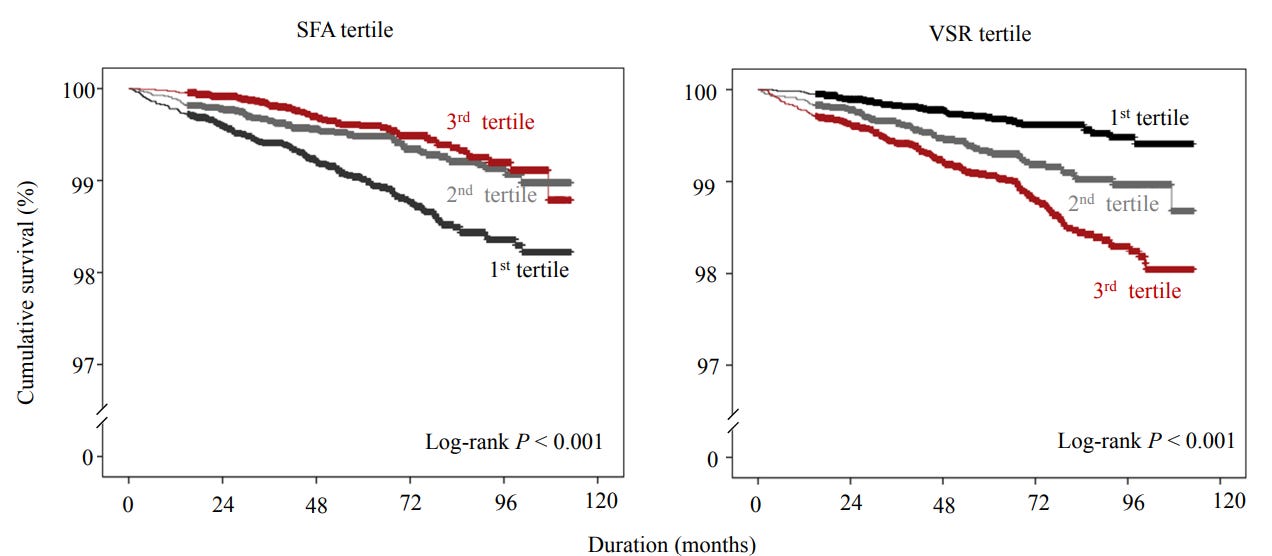
Nevertheless, it is still possible that the distribution of fat itself has a causal effect on health independent of overall adiposity. Within the few studies I have found that evaluate this, all of them agree that visceral fat (fat stored around the central organs) has a negative effect on health, and subcutaneous fat (fat underneath the skin) has either no effect or a protective one.
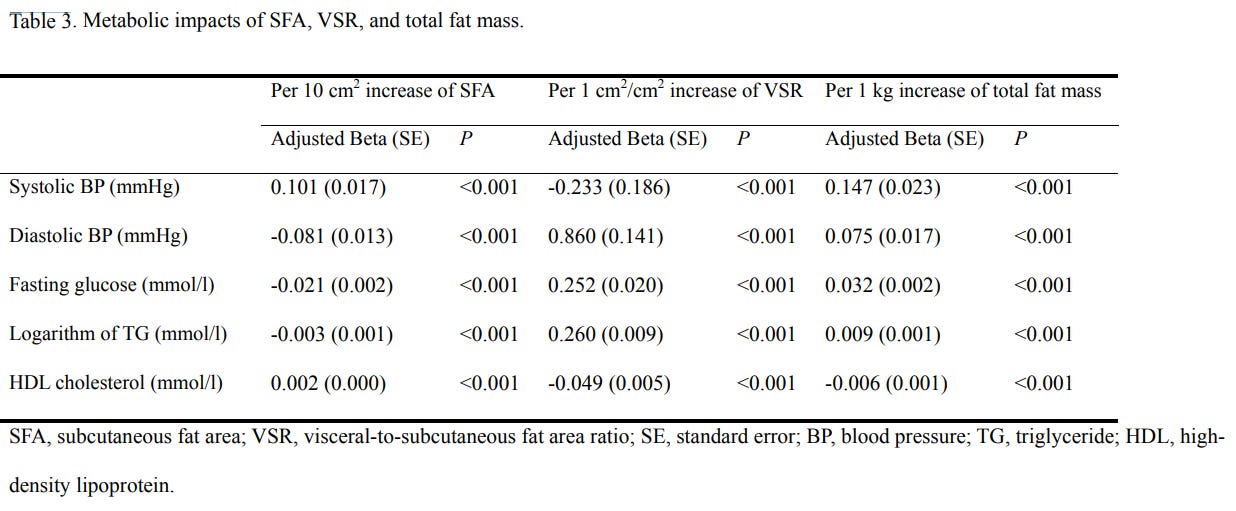
Subcutaneous fat, visceral fat, and fat mass are independently associated with different biomarkers as well - subcutaneous fat is associated with a larger differnece between systolic and diastolic blood pressure reading, lower fasting glucose, and higher HDL colesterol. On the other hand, visceral fat is associated with a smaller difference between systolic and diastolic blood pressures, higher levels of fasting glucose, and lower levels of HDL cholesterol.
There is still the problem of reverse causation, where severely ill people may be losing certain types of fat more than others, ideally this would be assessed with followup, but I have no data for this.
Unless you're full time body building influencer, there's no way you can "gain too much muscle" that'll be bad for your health. Most people don't lift. The ones that do lift regularly have regular jobs and are not taking performance enhancing drugs. It's not possible for a natty gym bro to build so much muscle that he has to be concerned about life expectancy of body builders.
Not building muscle is a health hazard especially when one gets old. Death from fall injuries is a big cause of mortality. And that's caused by not having good balance or grip strength because of weak muscles.
Looking at the chart it seems to tell you the relative stress index of those activities on the body beyond hormesis... constant protein shakes, constant creatine, constant pumping and upping. The latter activities at the end like horseriding and skiing don't seem to exert too much exogenous stress on the body when you think about it. Artistic gymnastics, fencing and whatnot are like short-burst activities -- not to mention shooting and the latter activities are confounded by wealthier quantiles of the population with low sizes. Basically the latter activities are characterized mostly by NEAT or intermediate activity, periodically like what we did in the past with tool-making, or whatever, an occasional hunt or two, sprint. Left hand side is more endurance-based, more strenuous, more repetitive.